
Why the 30-day manual claim follow-up cycle is dead — and what a FHIR-driven automated appeals pipeline actually does to claim recovery cost.
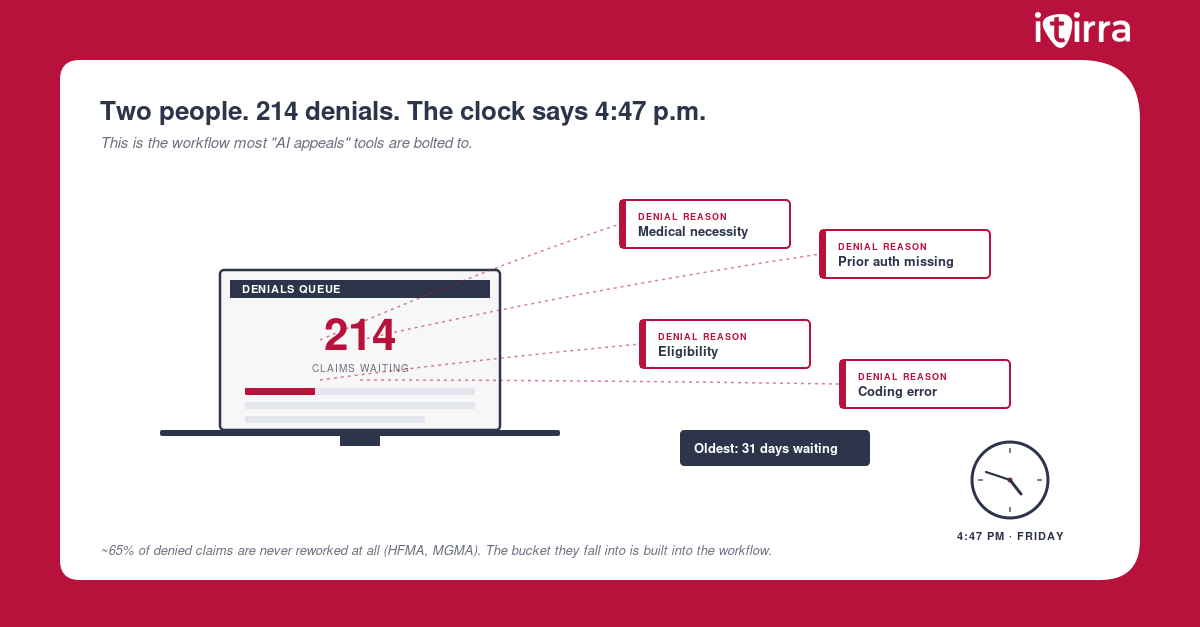
It’s 4:47 p.m. on a Friday. The appeals coordinator at a 180-bed community hospital opens her queue. There are 214 denials waiting. The oldest one was filed 31 days ago. The clinician who ordered the imaging study has been on a different rotation for three weeks. The chart is closed. The documentation is somewhere in a 47-page encounter note.
She has until next Friday to file the appeal. She is one of two people on the team.
This is what a manual claim follow-up cycle actually looks like in the wild. It is not a process problem. It is the process. And every health system running it is paying for the same workflow twice — once to generate the denial, and once to chase it down.
Vendors at HIMSS 2026 pitched “agentic AI for appeals” from the main stage. This Friday queue is what every health system buying that pitch is actually trying to fix.
There is a better architecture. This article is about what it looks like.
The Real Cost of Manual Appeals
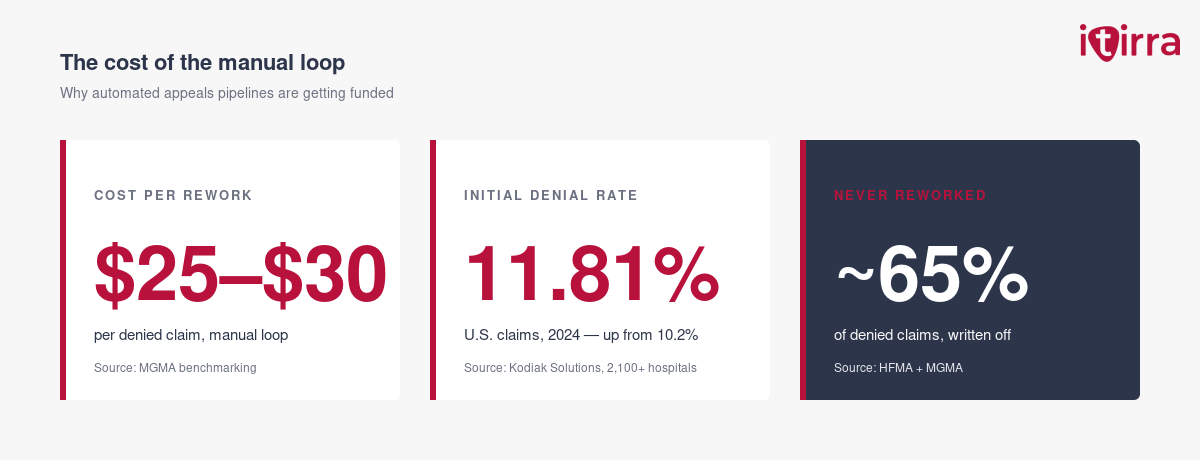
The headline number from MGMA’s 2024 benchmarking report is well known by now: each denied claim costs $25–$30 to rework and resubmit. That covers 50 to 70 minutes of biller or coder time, the supplies, the postage where appeals still ship by mail, and the overhead.
The headline number understates the picture.
A claim that goes through the full manual loop — denial received, denial categorized, chart reopened, clinician contacted, documentation re-extracted, appeal packet assembled, submitted, tracked, re-tracked — has a cycle time measured in weeks, not days. During those weeks, the denied dollars sit in unbilled or A/R-aged buckets. The cash flow penalty compounds.
Then there is the volume. Initial denial rates hit 11.81% in 2024 (Kodiak Solutions, on a benchmark of 2,100+ hospitals and 300,000+ physicians). The median final denial rate climbed from 2.5% in 2024 to 2.7% in 2025. Net revenue losses from final denials and bad debt grew by 25% across U.S. provider organizations in 2025 (Kodiak, March 2026).
Multiply 11.8% by your claim volume. Multiply that by $25–$30 per rework. Hold that against the share that never gets appealed at all because the team ran out of time. That is the manual loop. That is the cost center.
Why the Manual Loop Survives — and Why Bolting AI on Top Doesn’t Fix It
For a decade, the standard response to rising denial rates has been to add headcount in the appeals department. When that stopped scaling, vendors started selling “AI appeal letters” — large language models that draft a letter from the denial reason code and a prompt.
The buying activity is real. Becker’s 2025 CFO Outlook found 46% of healthcare organizations already using AI somewhere in revenue cycle, and another 49% planning to within twelve months. Most of that spend is going to letter-drafting and reason-code classification, not to integration. Which is why most of it will not move the denial rate.
A drafted letter is not an appeal. An appeal is a defensible packet of clinical evidence: the order, the indication, the relevant labs, the supporting note, the medical necessity argument tied to payer policy. Generating the prose is the cheap part. Assembling the evidence is what takes the 50 to 70 minutes per claim.
The manual loop survives because it is bolted to a structural gap: the EHR holds the clinical evidence, the billing system holds the claim data, the payer portal holds the denial reason — and none of them are wired to talk to each other at the moment a denial arrives. So a human becomes the integration layer. Every denial. Every time.
You cannot AI your way out of an integration problem. You can only architect your way out.
What an Automated Appeals Pipeline Actually Is
The term sounds like marketing. It is not. An automated appeals pipeline is a defined sequence of services that turns a denial event into a submitted appeal packet without a human re-extracting clinical documentation from the chart.
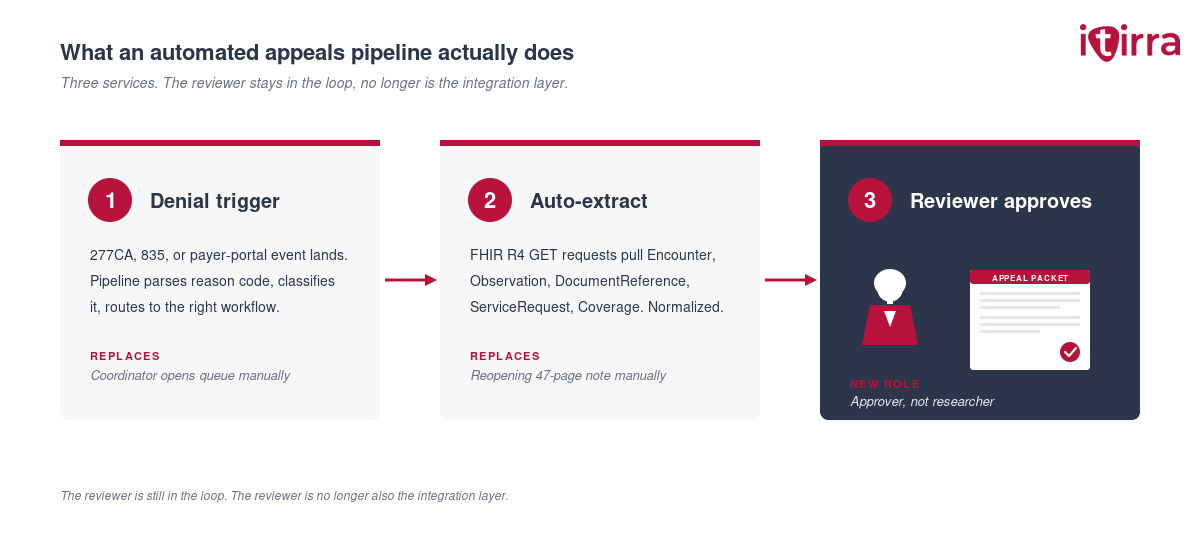
Three components, in order:
1. The denial trigger. A 277CA, 835, or payer-portal event lands. The pipeline parses the denial reason code and the claim line, classifies it (medical necessity, prior auth, coding, registration), and routes it to the right downstream workflow. No coordinator opens a queue. The system opens it.
2. Clinical evidence auto-extraction. This is where FHIR earns its keep. The pipeline issues GET requests against the source EHR’s FHIR R4 endpoints — Encounter, Observation, DocumentReference, ServiceRequest, Condition, Coverage — for the specific patient, encounter, and date range tied to the denied claim. It pulls the structured evidence the appeal needs into a normalized payload. No one reopens a 47-page note manually.
3. Packet assembly and submission. The normalized payload feeds a templating layer that maps payer-specific appeal formats. The clinical narrative is generated from structured fields, not invented. A reviewer sees a pre-assembled packet — evidence, narrative, payer policy reference, signature line — and either approves or edits in minutes. Submission goes through the existing clearinghouse or payer portal API.
The reviewer is still in the loop. The reviewer is no longer also the integration layer.
Manual vs. Automated: The Numbers
| Cost driver | Manual loop | Automated pipeline |
|---|---|---|
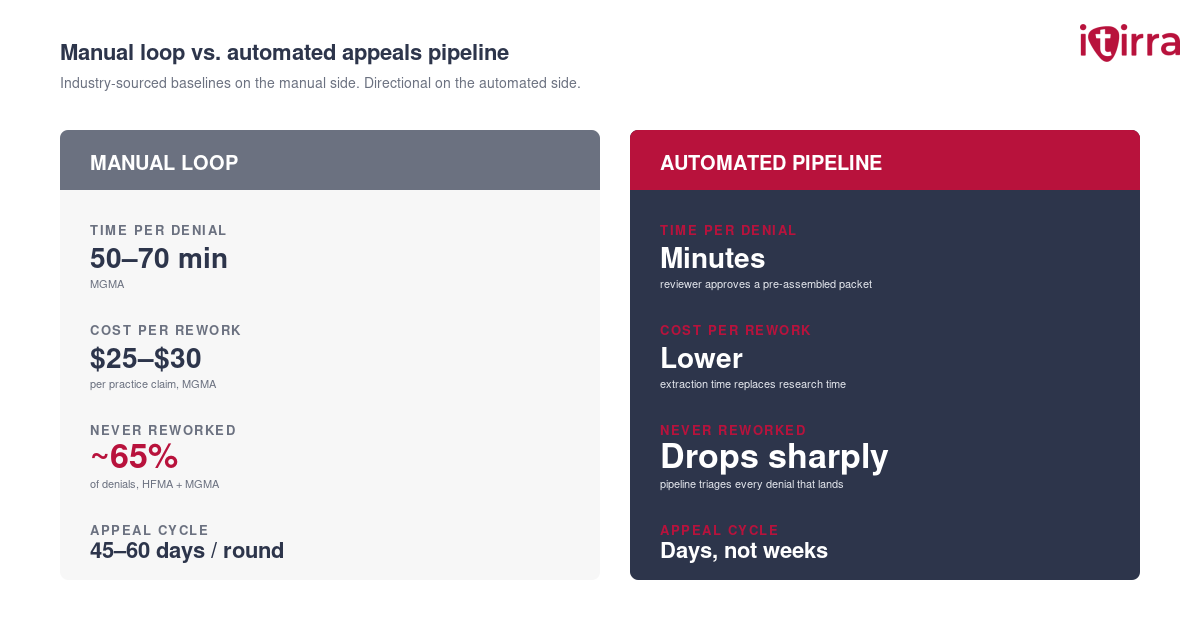
| Time per denial reviewed | 50–70 min (MGMA) | Minutes — reviewer approves a pre-assembled packet |
| Cost per claim reworked | $25–$30 per practice claim (MGMA); higher for hospital-side | Lower per claim — extraction time replaces research time |
| Share of denials never reworked | ~65% — HFMA and MGMA (industry “never-worked” rate) | Drops sharply — pipeline triages every denial that lands |
| Internal-appeal cycle | 45–60 days per round, often three rounds (KFF, ACA marketplace data) | Days — packet is ready as soon as the denial is parsed |
| Documentation re-extraction | Manual chart dive | FHIR auto-pull |
| Appeal letter drafting | Manual or templated | Generated from structured evidence |
| Reviewer role | Researcher + writer + filer | Approver |
The single most expensive number on this table is the one most teams stop talking about: roughly 65% of denied claims are never reworked at all (HFMA, MGMA). That share is not a process inefficiency. It is revenue written off because the manual loop ran out of time. A pipeline that triages every denial and assembles the evidence automatically is what moves that bucket from “written off” to “worked.”
These are not vendor-marketing numbers. They are the published industry baselines — and the math of what changes when the integration layer stops being a person.
How the Pipeline Gets Built
Most health systems can build this without ripping out a single existing system. The pipeline is an integration layer on top of what is already in place. The phasing matters more than the technology stack.
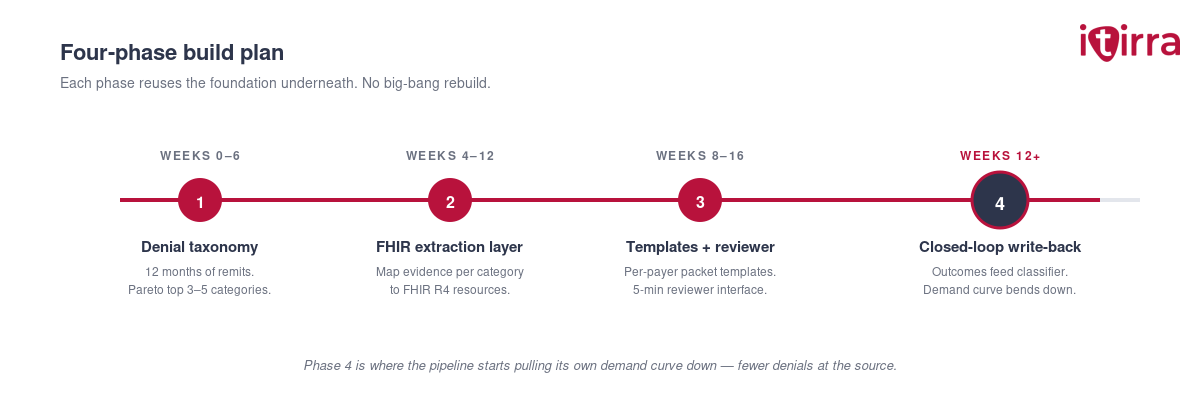
Each phase reuses the foundation underneath. No big-bang rebuild.
Phase 1: Denial taxonomy and high-impact triage (Weeks 0–6).
Pull the last twelve months of remits. Classify denials by reason code, payer, service line, and dollar value. The Pareto curve will be obvious — usually three to five denial categories drive 70 to 80% of recoverable dollars. The pipeline gets built for those categories first, in priority order. Do not boil the ocean.
Phase 2: FHIR extraction layer (Weeks 4–12).
The major EHRs already expose FHIR R4 endpoints. The build is mapping the appeal-evidence requirements (per denial category, per payer) to the right FHIR resources, then standing up a service that normalizes responses across endpoints. Design for new payer rules to land as configuration changes — not new code paths. You will be glad of this on payer number four.
Phase 3: Packet templates and reviewer workflow (Weeks 8–16).
Per-payer appeal templates with merge fields for the FHIR-extracted evidence. The reviewer interface is where the time savings live — design it so a reviewer can approve, edit, or reject in under five minutes per packet. Audit trail and signature capture are not optional; they are how this survives an external audit.
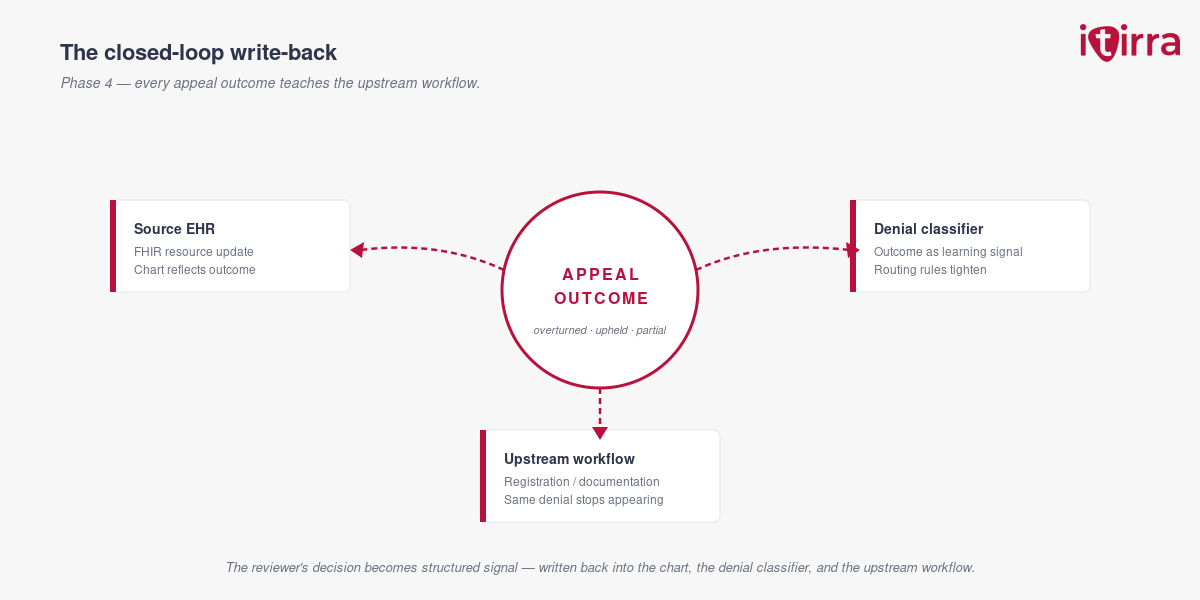
Phase 4: Closed-loop write-back (Weeks 12+).
Every appeal outcome — overturned, upheld, partial — gets written back into the source systems as a FHIR resource update and into the denial classifier as a learning signal. The pipeline that filed the appeal also tells the upstream workflow what to fix so that denial category stops generating new claims. This is where the appeals pipeline starts pulling its own demand curve down. (For more on the upstream loop, see why bolting AI onto a broken RCM workflow doesn’t move the denial rate.)
Common Mistake: Treating the pipeline as a back-office IT project. The owners must be revenue integrity, clinical informatics, and integration together. If the people who understand the appeal evidence requirements are not in the design room, the FHIR extraction will pull the wrong fields and reviewers will lose trust in the packets.
Consultant’s Tip: Pick the highest-volume denial category your team already understands well, and build the first vertical of the pipeline end-to-end before adding a second category. A working narrow pipeline is more valuable than a half-built broad one — and the team learns the operating model on the easy case before the hard ones land.
What Changes When the Pipeline Goes Live
The CFO sees three things move within two quarters. The “never-worked” denial bucket shrinks — every denial that lands gets triaged and an evidence packet, not just the ones the team has time for. Appeal cycle time on the denials that do get filed compresses, because the multi-week chart-dive step is no longer in the middle of it. Direct rework cost per claim drops as reviewer time replaces researcher time. The recovered-revenue line moves more slowly, then accelerates as Phase 4 write-back starts pulling denial volume down at the source.
The clinical side sees something different. Department heads stop getting paged about claim documentation gaps from six weeks ago. Coders stop sending the same query for the third time on the same case. Appeals coordinators stop being the integration layer.
Let doctors be doctors. Let coders code. Let the integration handle the paperwork.
The 30-day manual follow-up cycle is not an artifact of how revenue cycle has to work. It is an artifact of the architecture under it. Replace the architecture and the cycle disappears.
The Takeaway
The appeals process is expensive. Manual. And mostly avoidable.
Most of what makes it expensive is the integration gap between systems that already hold the evidence the appeal needs. An automated appeals pipeline closes that gap with FHIR-based extraction, structured packet assembly, and a reviewer workflow that turns researchers and writers into approvers.
That is what moving RCM from a cost center to a revenue engine actually looks like. Not a smarter scrubber. Not another AI pilot. A pipeline that does the integration work humans were never the right tool for.
That is the architecture we build at Itirra.
Is your appeals team carrying the integration layer in their heads? Let’s talk about your project.
Sources
- MGMA — denials & appeals benchmarking: $25–$30 cost per denied claim to rework, 50–70 minutes of staff time per appeal, ~65% of denied claims never reworked. mgma.com
- HFMA — Redesigning denials management in the OBBBA era: confirms ~65% of denials never re-worked; HFMA Claim Integrity Task Force standardized denial metrics for benchmarking. hfma.org
- Kodiak Solutions RCM Benchmarking, 2024 data: initial denial rate of 11.81% in 2024, up from 10.2% in 2020. businesswire.com
- Kodiak Solutions RCM Benchmarking, 2025 data: median final denial rate up from 2.5% to 2.7%; net revenue losses from final denials and bad debt grew 25% in 2025. businesswire.com
- KFF — Claims Denials and Appeals in ACA Marketplace Plans in 2024: internal-appeal cycle data, 45–60 days per round, multi-round structure. kff.org
- Becker’s Hospital Review — 2025 CFO Outlook: 46% of healthcare organizations already using AI in revenue cycle, 49% planning to within twelve months. beckershospitalreview.com
- HL7 FHIR R4 specification: Encounter, DocumentReference, Coverage, Observation, ServiceRequest resources used in evidence extraction. hl7.org/fhir/R4/
- HL7 Da Vinci Project — CRD and DTR Implementation Guides: payer/provider FHIR appeals workflow. hl7.org/about/davinci/